Potential toxicity from use of Gadolinium based contrast media.
What is gadolinium (Gd)?
Gd-based contrast agents (GBCAs) have been widely used as magnetic resonance imaging (MRI) contrast media since the late 1980’s. The paramagnetic properties of the GBCA’s enhance signal intensity through the shortening of the time taken to temporarily magnetise nuclei (within tissue) in the direction of magnetic field and consequently improve the visibility of internal organs, blood vessels and tissues.
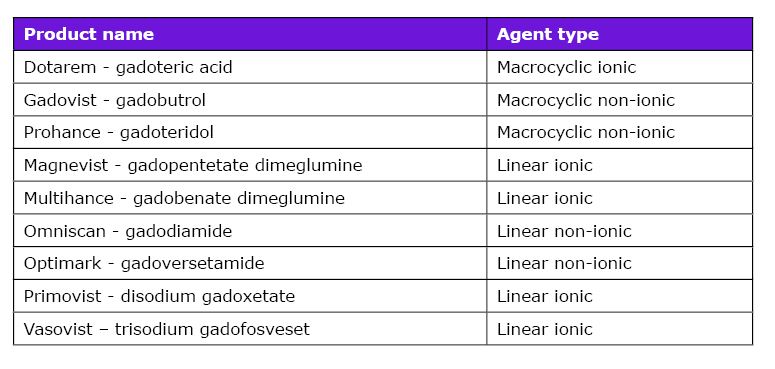
To date, nine GBCA’s have been used globally for clinical use (see table below) and are classified into two groups, based on structure of the ligand binding. In the ‘macrocyclic’ group, the Gd3+ ion is caged within a pre-organised cavity of the ligand, whereas in the ‘linear’ group, the ligand has linear geometry (open chain). Each category can in turn be subdivided into ionic (dissociates/dissolves as charged particles in solution) or non-ionic, based on charge. The macrocyclic molecule is less likely to release the Gd3+ ion (which is toxic in the ‘free’ form) and is thus more stable than the linear form, whilst the ionic linear chelates are more stable than the linear non-ionic chelates.
The link between GBCA’s and nephrogenic systemic fibrosis
Until about a decade ago, the GBCA’s were believed to be rapidly excreted in intact form, and thus considered safe to use at recommended doses in subjects with normal renal function. However, an association between the administration of GBCA (and linear contrast agents in particular) and the development of a rare, but severe condition Nephrogenic Systemic Fibrosis (NSF) was described in 2006 in patients with renal insufficiency(1). NSF is associated with widespread progressive tissue fibrosis arising from the deposition of fibroblasts and collagen: the aetiology is believed to be the release of gadolinium ions from the chelated complex(es) due to impaired clearance. Limiting the use of GBCAs in patients with renal failure and encouraging the use of more stable GBCA’s (and at low doses), has resulted in a marked fall in NSF cases.
More recent reports have however, emerged indicating that gadolinium may be retained in various tissues of the human body (including brain, kidneys and bone) even in patients with normal renal function, leading to neurological, musculoskeletal and dermal consequences(2). Retention is higher in patients receiving multiple MRI scans. Studies in animals have similarly demonstrated increased tissue deposition of Gd following exposure to GBCA’s. There is currently no consensus regarding the clinical significance of accumulation (and potential mechanism for toxicity) and treatment of gadolinium accumulation. Thus the FDA has asked manufacturers of these GBCA’s to conduct human/animal studies to assess their safety.
Case Study:
Gd concentrations were measured in urine samples obtained from a 50 year old male patient who had had exposure to Gadovist contrast medium (macrocyclic, non-ionic) MRI, every 4-6 months since August 2011 and every quarter for the last two years, for a brain glioma. The renal function in the subject was normal during this period. Gd concentrations were measured in samples obtained pre-, during and post chelation with the chelating agent succimer (Dimercaptosuccinic acid, DMSA), that is commonly used in the treatment of lead, mercury and arsenic poisoning.
Gd was measured in Viapath’s Trace Element laboratory using Inductively Coupled Plasma Mass-Spectrometry in standard mode and using rhodium as the internal standard. Concentrations were corrected for creatinine.
Gd excretion was significantly elevated (~75-fold) in samples collected during chelation therapy with DMSA. Increased excretion was still evident 2 days after chelation therapy had been halted. Excretion seemed to normalise 9-10 days after chelation therapy.
These measurements provide evidence of gadolinium build up following MRI scans. However it is unclear if the Gd accumulation is in the free form (Gd3+) or in association with ligand(s). It is feasible that the accumulation could contribute to clinical complications.
For further information, please contact
Kishor Raja
Kishor.raja [at] nhs.net
References:
1. Marckmann P. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol. 2006. 17; 2359-62
2. Ramalho J et al. Gadolinium-Based Contrast Agent Accumulation and Toxicity: an update. Am J Neuroradiol. 2016, 37; 1192-98